# Do nothing2 フレイル
2.1 フレイルの定義
フレイルについての重要な論文は、さまざまな検索をした結果、以下の 3 つに絞ってみました。1
1 PubMed または Google Scholar を使い、frailty について検索してみなさい。
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, … & McBurnie MA (2001) Frailty in older adults: evidence for a phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 56(3), M146-M157.
- Clegg A, Young J, Iliffe S, Rikkert MO, & Rockwood K (2013). Frailty in elderly people. The Lancet, 381(9868), 752-762.
- Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, & Mitnitski A (2005) A global clinical measure of fitness and frailty in elderly people. CMAJ, 173(5), 489-495.
さて、これらのなかで必ず読むべき論文はどれか?と聞かれたら、全てです。その中で一つというならば、おそらく Clegg A (2013) The Lancet となります。比較的新しいのと、ジャーナルが有名という点です。
ただし、ここでは Fried LP (2001) The Journals of Gerontology Series A2 を読んでみたいと思います。理由としては、フレイルの定義としてもっとも定着している Phenotype 法を提唱した論文だからです。Fried LP (2001) の中身そのものが医師国家試験で出題されたことがあります。
2 The Journals of Gerontology Series A とは、どのようなジャーナルか?
Note第113回 F 27
身体的フレイルの評価基準として誤っているのはどれか。
a 易疲労感
b 握力の低下
c 睡眠時間の短縮
d 歩行速度の低下
e 日常生活活動量の低下
この問題の正解を知るために、以下の論文を読んでみましょう。
2.2 論文
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, … & McBurnie MA (2001) Frailty in older adults: evidence for a phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 56(3), M146-M157.
https://doi.org/10.1093/gerona/56.3.m146
著者はたくさんいますが、第一著者は Linda P. Fried で、当時の所属 (affiliation) は The Johns Hopkins Medical Institution でした。3
3 What is her current affiliation?
この論文はオープンアクセスではないので、Abstract と Figure 3 のみ読みます。本文全体 (Figure 3 を含む) は、Universal Passport などから入手してください。
2.3 Abstract
Abstract は、構造化されています。
Background. Frailty is considered highly prevalent in old age and to confer high risk for falls, disability, hospitalization, and mortality. Frailty has been considered synonymous with disability, comorbidity, and other characteristics, but it is recognized that it may have a biologic basis and be a distinct clinical syndrome. A standardized definition has not yet been established.
背景 フレイルは老年期に多くみられ、転倒、障害、入院、死亡のリスクが高いと考えられている。フレイルは、障害、重複疾患、その他の特徴と同義であると考えられてきたが、生物学的基盤があり、明確な臨床症候群である可能性が認められている。標準的な定義はまだ確立されていない。
disability: 障害
prevalent: 流行している; prevalence は有病率
fall: 転倒
hospitalization: 入院
comorbidity: 複数の疾患を抱えている状態、重複疾患
Methods. To develop and operationalize a phenotype of frailty in older adults and assess concurrent and predictive validity, the study used data from the Cardiovascular Health Study. Participants were 5,317 men and women 65 years and older (4,735 from an original cohort recruited in 1989–90 and 582 from an African American cohort recruited in 1992–93). Both cohorts received almost identical baseline evaluations and 7 and 4 years of follow-up, respectively, with annual examinations and surveillance for outcomes including incident disease, hospitalization, falls, disability, and mortality.
方法 高齢者におけるフレイルの表現型を作成・運用し、同時性と予測妥当性を評価するために、本研究では心血管健康調査(Cardiovascular Health Study)のデータを用いた。参加者は65歳以上の男女5,317人(1989-90年に募集されたオリジナルコホートから4,735人、1992-93年に募集されたアフリカ系アメリカ人コホートから 582 人)であった。両コホートは、ほぼ同じベースライン評価を受け、それぞれ 7 年間と 4 年間のフォローアップを受け、年 1 回の検査と、疾病の発生、入院、転倒、障害、死亡を含む転帰のサーベイランスを受けた。
operationalize: to define an abstract concept in concrete, measurable terms so that it can be observed, measured, and analyzed in a study. 心理学などでよく用いられる。
incident: 発症
Note
Fried LP によるフレイル定義は、
- 表現型 (Phenotype)
- CHS 基準
などと呼ばれます。
Results Frailty was defined as a clinical syndrome in which three or more of the following criteria were present: unintentional weight loss (10 lbs in past year), self-reported exhaustion, weakness (grip strength), slow walking speed, and low physical activity. The overall prevalence of frailty in this community-dwelling population was 6.9%; it increased with age and was greater in women than men. Four-year incidence was 7.2%. Frailty was associated with being African American, having lower education and income, poorer health, and having higher rates of comorbid chronic diseases and disability. There was overlap, but not concordance, in the cooccurrence of frailty, comorbidity, and disability. This frailty phenotype was independently predictive (over 3 years) of incident falls, worsening mobility or ADL disability, hospitalization, and death, with hazard ratios ranging from 1.82 to 4.46, unadjusted, and 1.29–2.24, adjusted for a number of health, disease, and social characteristics predictive of 5-year mortality. Intermediate frailty status, as indicated by the presence of one or two criteria, showed intermediate risk of these outcomes as well as increased risk of becoming frail over 3–4 years of follow-up (odds ratios for incident frailty = 4.51 unadjusted and 2.63 adjusted for covariates, compared to those with no frailty criteria at baseline).
結果 フレイルは、
- 意図しない体重減少
- 自己申告による疲労
- 筋力低下(握力)
- 歩行速度の低下
- 身体活動低下
のうち 3 つ以上が認められる臨床的症候群と定義された。
この地域住民集団におけるフレイルの全有病率は6.9%であり、年齢とともに増加し、男性よりも女性で大きかった。
観察研究は、比較級の宝庫です。
It (Frailty) … was greater in women than men.
There was overlap, but not concordance, in the occurrence of frailty, comorbidity, and disability.
フレイル、重複障害、障害の併発には、一致はしていないが重なりがあった、とあります。ここは、本文の Figure 3 で解説します。
結果として、フレイルは以下のように定義されました。
- unintentional weight loss (10 lbs in past year)
- self-reported exhaustion
- weakness (grip strength)
- slow walking speed, and
- low physical activity
このうち 3 つ以上当てはまると「フレイル」となります。では、国家試験の問題に戻りましょう。
Note第113回 F 27
身体的フレイルの評価基準として誤っているのはどれか。
a 易疲労感
b 握力の低下
c 睡眠時間の短縮
d 歩行速度の低下
e 日常生活活動量の低下
誤っているのは、c となります。
Conclusions. This study provides a potential standardized definition for frailty in community-dwelling older adults and offers concurrent and predictive validity for the definition. It also finds that there is an intermediate stage identifying those at high risk of frailty. Finally, it provides evidence that frailty is not synonymous with either comorbidity or disability, but comorbidity is an etiologic risk factor for, and disability is an outcome of, frailty. This provides a potential basis for clinical assessment for those who are frail or at risk, and for future research to develop interventions for frailty based on a standardized ascertainment of frailty.
結論 本研究は、地域居住高齢者におけるフレイルの標準化された定義の可能性を提供し、その定義に対する同時妥当性と予測妥当性を提示するものである。また、フレイルのハイリスク者を特定する中間段階が存在することも明らかにした。最後に、フレイルは合併症や障害と同義ではなく、合併症はフレイルの病因となる危険因子であり、障害はフレイルの結果であるという証拠を示している。このことは、フレイルまたはその危険性のある人の臨床評価や、標準化された虚弱の把握に基づいたフレイルへの介入を開発するための今後の研究の基礎となる可能性を示している。
これにより、
重複疾患 \(\rightarrow\) フレイル \(\rightarrow\) 障害
という流れが判明しました。
2.4 Figure 3
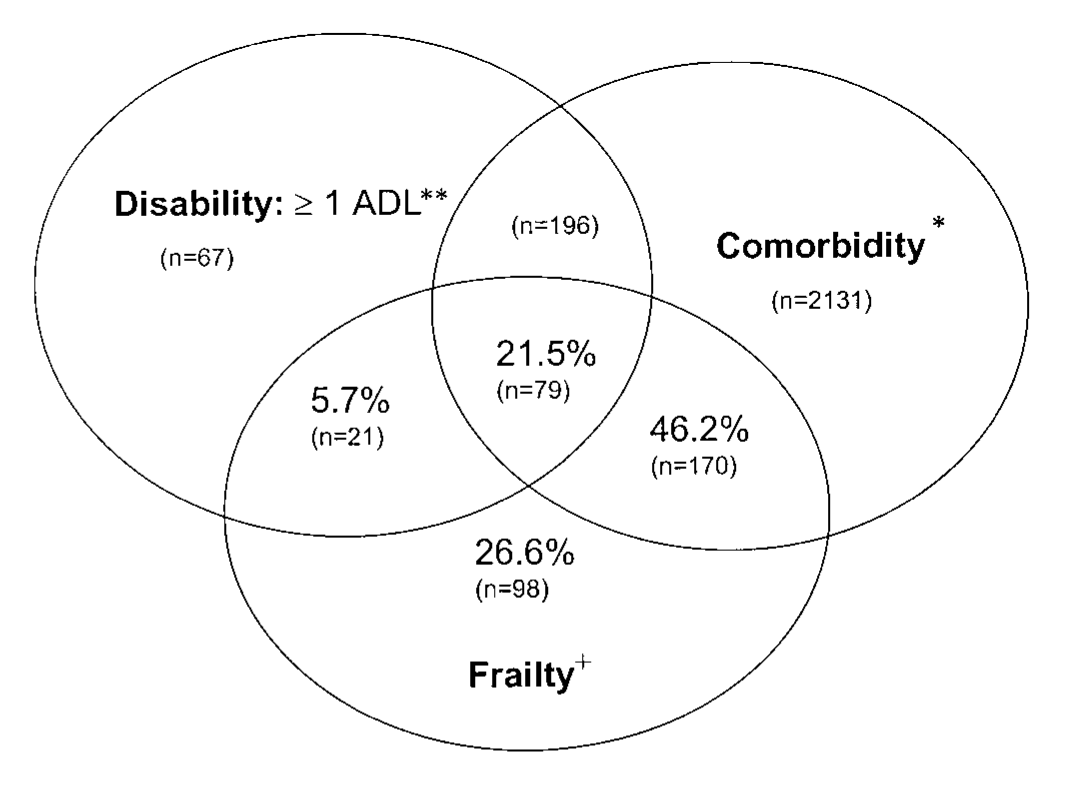
この図はベン図と呼ばれるもので、数学の集合などでよく登場します。
Fig. 3 displays the overlap between these characteristics, as well as with the presence of two or more comorbid diseases. There was only modest concordance between frailty and disability. Of those who were frail, 46% had comorbid disease, 6% had ADL disability, 22% had both comorbid disease and ADL disability, and 27% had neither ADL disability nor comorbidity.
図 3 は、これらの特徴間の重複と、2 つ以上の併存疾患の有無を示している。虚弱と障害の間には、わずかな一致しか見られなかった。虚弱であった人のうち、46%に併存疾患があり、6%にADL障害があり、22%に併存疾患とADL障害の両方があり、27%にADL障害も併存疾患もなかった。
割合は、フレイル以外の人は除外し、フレイルの人 (21 + 79 + 170 + 98 = 368) を母数とした割合になっています。
重複疾患 (comorbidity) を持っている人は、79 + 170 = 249 人です。割合は、249/368 = 68% のはずですが、ここでは重複疾患を持っておりADL障害を持っていない 170/368 = 46% と報告しています。ここはちょっと不正確な印象があります。